
This questionnaire was adapted as part of the actions for the National Food and Nutrition Surveillance (FNS) program [12]. The methodology of this study was completely described elsewhere [13]. Additional explanations are briefly given here.
Adaptation of a questionnaire to nutritional diversity
The questionnaire was adjusted for this study. According to the guidelines defined by the FAO, a 12-question questioning questionnaire (can be found in additional files) was adjusted to estimate the dietary variety in children. This questionnaire, which is known as DDQ, recorded the day before children who are consumed by children. In order to ensure cultural relevance and inclusion in locally consumed food, the DDQ was adapted to household foods in the existing categories of the food group. In accordance with the guideline, food was divided into nine groups. Food groups, subgroups and their examples involved in DDQ were shown in the addition table.
Food quantities that correspond to or exceed a tablespoon (≥ 15 g) were included in the score calculation. We then calculated the DDS as the sum of all food groups consumed by each child, with a total number of points between 1 and 9. DDS is calculated by adding up the number of food groups consumed by the child in the last 24 hours.
Sampling
In order to determine the sample size, α- and β errors were viewed as 5% or 10%. Consideration of previous research [14]The correlation coefficient between the middle adequacy ratio (Mar) and DDS was expected to be 0.4. Using these parameters, the calculated sample size was 408 children.
Recruitment and authorization examination
Children aged 24 to 59 months were entitled to admit this study. The exclusion criteria included reluctance in participation, the presence of physical and/or mental impairments and compliance with special diets.
In each province, a multi -stage cluster was carried out proportional to the size (PPS). The steps were as follows:
-
A
A combination of small neighboring cities was considered a primary sampling unit (PSU). A list of psus based on a geographical location and municipal stories together with their population figures. Systematic random pps samples were then selected.
-
B
Cities and villages were treated as secondary sampling units (SSU). A list of SSUs, including cities and villages with their respective population, was created for each PSU selected in the previous phase. SSUs were selected by each PSU using a systematic random pps sample.
-
C
Households were shown as list units. The sampling within cities and villages was carried out using a simple random method based on postcodes. The postcodes were divided into Executive clusters exclusively for the management of stab -made teams. They were not statistical clusters.
-
D
Each participant between the ages of 2 and 5 was seen as an elementary unit. From each selected household, authorized subjects were selected in the required age and gender sub-groups for the program for monitoring food and nutrition (FNS) with a simple random method.
Each executive cluster consisted of 20 samples. All legitimate subjects were enrolled from each household within the specified age and gender sub-groups. The position of each cluster was determined by identifying the address of the cluster head using a 10-digit postcode. These addresses were received by IR Iran Post Company. The sampling began from the cluster head, and by the right side and the selection of the following households, the sample process continued until the required sample size was reached. The flow of study population can be found in Fig. 1.
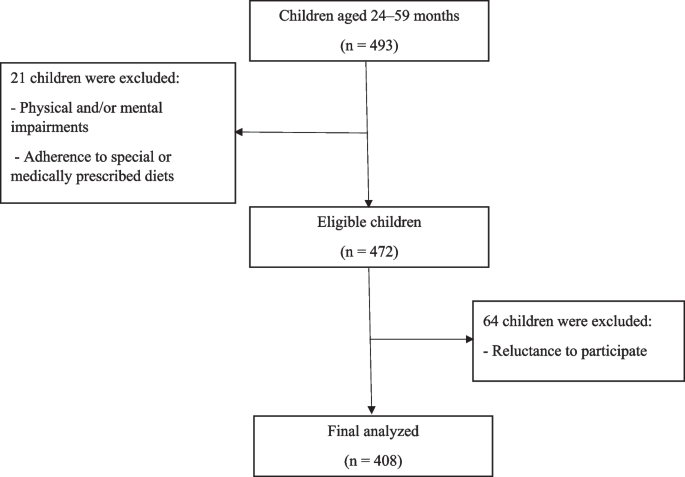
The flow diagram of the study population
Data acquisition
We used two different methods for collecting information: a mobile application and an electronic questionnaire. A custom Android application was specially developed to collect the demographic, biochemical and anthropometric data. The online questionnaire was available for the completion of the questions about nutritional diversity. The interviewers (healthcare staff) were allowed to access this questionnaire via a web -based platform. Several webinar workshops were held in order to train the interviewers, both for filling out the questionnaire and using the application (i.e. installation, work, error correction and daily sending of data). After each workshop, the data providers worked with the app, filled out the questionnaires and transmitted the data in 2 to 3 days. In this way, they familiarized themselves with the questionnaire and the app, and possible problems that they may have met were dissolved.
Anthropometric measures
Weight and size were measured for each participant using a calibrated scale or stadiometer. The weight was measured to 100 g, with the test subjects wearing light clothes and without shoes. The height was measured to 0.5 cm. Height for age (HAZ), weight for age (WAZ), weight for the height (WHZ) and BMI-for-Age (BAZ) Z-Scores, according to the World Health Organization (WHO), instructions in 2006 were calculated [15].
Nutritional assessment
The DDQ was completed by the parents/caregivers of the children. Two non-consecutive 24-hour calls for nutrition were completed in order to collect the recording data of the diet by each participant. The two 24-hour recalls were collected by direct interviews with the parents or supervisors. The recalls were administered by trained interviewers with a questionnaire with detailed information on consumed foods, portion sizes and cooking methods. The consumed foods were initially converted into grams, according to which the nutrients and energy content were calculated using the Nutritionist IV software and the US Ministry of Agriculture (USDA) food composition table (FCT). To analyze local foods, we also used an Iranian FCT [16]. The information on local foods was inserted into the software for nutritionists by the command “Food Add Food”. All phases were carried out by experienced and trained nutritionists.
Nutritional adequence
The nutrient requirements were used to determine the nutrient adequency by comparing the children. The nutrient adequency was assessed by calculating the ratio of nutrient adequacy (NAR) for energy, protein and 12 micronutrients (vitamin A, vitamin E, b1B2Niacin, born6B12Folic acid, vitamin C, calcium, iron and zinc). The NAR was calculated by dividing the actual nutrient absorption by the estimated average requirement (OS) for each nutrient. Since there was no current information about the bioavailability of iron and zinc in the investigated community, we reported to report all bio -availability levels based on the reference of the WHO [16]. The average adequacy ratio (Mar) was also calculated, which represents the average NAR across all nutrients. For both NAR and MAR, an admission-to-limitation ratio of 100% was considered optimal, since the recording was precisely aligned with the requirement. The energy, protein, vitamin and mineral requirements for every gender and age group were calculated based on the ear.
Biochemical evaluation
Five milliliters of not almost venous blood, which was taken from each child, were transferred to a fresh test tube that was covered by an aluminum foil. Blood samples were kept in a cold box during transport to the local health center. Then blood samples were centrifuged for 30 minutes at room temperature (RT). The serums were separated and aliquoted in clean microt theses and then held at 20 ° C. All serum samples were transported to the laboratory for nutritional research at the National Nutrition and Food Technology Research Institute (NNFTRI) in order to obtain further analyzes while the cold chain was maintained. Serum -Retinol was measured using HPLC, as described elsewhere [17].
Ethical questions
All parents/supervisors signed a declaration of consent after a comprehensive review of the inclusion and exclusion criteria and a detailed explanation of the study protocol. The study protocol was approved by the Ethical Committee of the National Research Institute of the National Nutrition and Food Technology, Shahid Beheshti University of Medical Sciences (IR.SBMU.NNFTRI.REC.1401.025).
Statistical analysis
The data was analyzed with the Stata software (version 18). Descriptive statistics were used to summarize demographic features. Continuous variables were expressed as a mean ± standard error (SE). Categorical variables were expressed as frequencies and percentages. The normality of continuous variables was assessed using the Shapiro Wilk test. Independent sample t-tests or man-whitney U tests were used to compare the funds for continuous variables between boys and girls. Chi square tests were used to evaluate the connection between categorical variables.
The correlation analysis was used to evaluate the relationships between DDS and nutrient -adequate indicators, including NARS, Mar and other variables. It was reported that correlation coefficients and P values determine the strength and significance of these associations. The logistical regression analysis was carried out to evaluate the connection between DDS and the risk of stunt, underweight and waste. Adjustments were made for potential disruptive factors, including age, gender.
The sensitivity and specificity of DDS when predicting the nutritional adequacy (using Mar as a criterion) was evaluated at various DDS limit points. The ROC curve analysis (recipient operating properties) was carried out to determine the optimal DDS limit value, which maximized both sensitivity and specificity. The area under the ROC curve (AUC) was calculated in order to quantify the overall ability of DDS between adequate and inadequate nutritional status. An AUC of 0.5 does not indicate a discriminatory ability, while an AUC of 1.0 shows perfect discrimination. A P value of less than 0.05 was considered statistically significant for all tests.